
The treatment of clubfoot using the Ponseti Method requires continuous patient assessment and functional evaluation, more so in children of walking age. These essential processes help to plan treatment (manipulation, casting, tenotomy and bracing) as well as determine treatment outcomes. At times, when clinical and functional assessment identify patients with poor treatment outcomes or relapse of the clubfoot deformity, further referral to orthopaedic specialists for review or surgical intervention may be necessary. In low resource settings where there are a limited number of orthopaedic specialists, consultation for further management is difficult. In such instances clinical photography can be a useful alternative to physical visits and in-person assessment. As a key component of telemedicine, photographs can make remote evaluation of treatment outcomes and planning of future interventions possible.
We conducted a study in 2017 to determine the diagnostic performance of photography in assessing clubfoot treatment outcomes for a cohort of children with idiopathic clubfoot treated between 2011 and 2013 in Harare, Zimbabwe. Here we will outline the methods used and give a summary of our findings. We will also point out the lessons learnt while using digital photographs in our study.
We assessed the participants using the Assessing Clubfoot Treatment (ACT) which is a tool that scores responses to each of the following questions on a scale from 0-3.
i) Is the foot plantigrade?
ii) Does the child complain of pain in the affected foot?
iii) Can the child wear shoes of their choice?
iv) How satisfied a parent/caregiver is with the child’s foot?
Scores for the responses were added up, giving a total from 0 to 12 where 12 is the ideal result. Patients with an ACT score of 11 or more were determined to have had a successful treatment outcome. Those with a total score of 8 or less were classified as having failed treatment and needing further treatment and referral. Those who scored between 9 and 10 were classified as having a borderline treatment outcome.
We went on to take 3 photographs of the children’s lower limbs to check for residual hindfoot varus and the degree of passive dorsiflexion (residual equinus deformity) in a child’s ankle. For the latter, 2 photographs were taken, one with each patient in supine with knees extended and another with the patient in standing with knees flexed. Photographs were then independently viewed by 2 blinded orthopaedic surgeons who used goniometers to assess the relevant angles on their laptops and determined the need for further orthopaedic review.
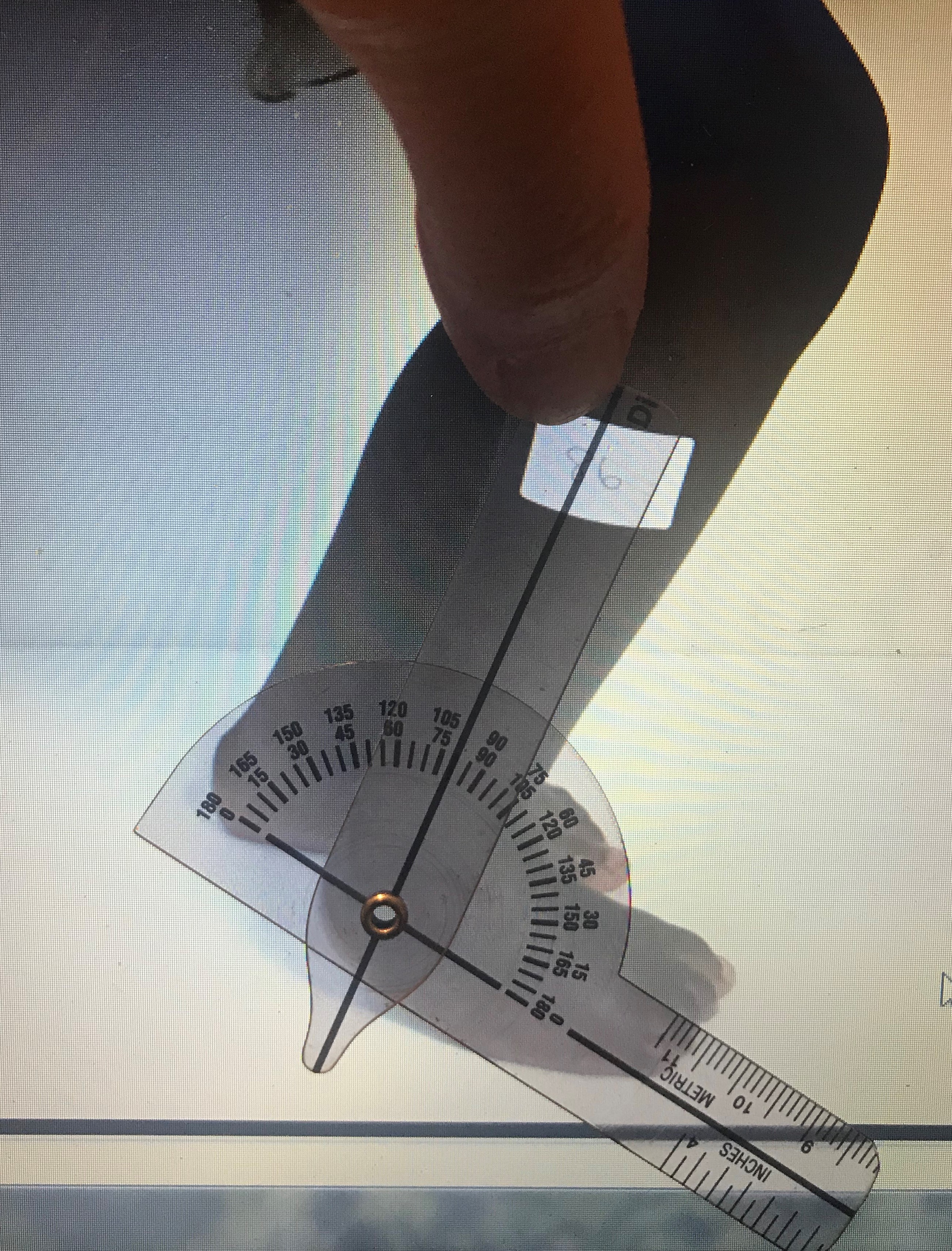

(c) Images courtesy of Marie-Caroline Nogaro
Results and lessons learnt
The main finding was that digital photographs could be easily used to help to confirm, but not exclude, success of clubfoot treatment. It was easier to recognise a well-corrected foot and a foot with clear residual clubfoot deformity, rather than one which was partially improved (borderline) via digital photography. In addition, photographs of feet with some residual deformity did not necessarily warrant further referral for specialist orthopaedic treatment. Though there was fair correlation between outcome of clubfoot treatment using the ACT scores and photographic evaluation we also learnt the following in our study.
- Clinical photographs need to be clear and of good quality for them to be valuable. If they have a low resolution, any blurring or poorly defined anatomical markings, the recipients may fail to interpret them accurately.
- There should be optimal lighting and background contrast so that pictures are clear and easy to read. For instance, when taking photos of a dark skinned patient against a dark background, the pictures will not come out clearly.
- There is need to develop clear instructions on how to take clinical photographs e.g. whether position a patient in supine, standing or squatting, to allow repeatability and comparison.
- Standardization of assessment parameters is key to avoid suboptimal patient positioning e.g. assessment of ankle dorsiflexion (residual equinus) with the knees in full extension.
- Well corrected feet (successful outcome) and those with clear residual deformities (failed outcome) are easily identified using photographs, however partially corrected feet are difficult to depict from photos.
Clinical photographs can be useful in determining if feet are well corrected or require further surgical or other intervention. There is however room to improve how photographs are taken and interpreted when assessing clubfoot treatment and outcomes.
Resources
Smythe, Tracey; Nogaro, Marie-Caroline; Clifton, Laura J; Mudariki, Debra; Theologis, Tim; Lavy, Chris; (2020) Remote monitoring of clubfoot treatment with digital photographs in low resource settings: Is it accurate? PloS one, 15 (5). e0232878-. DOI: https://doi.org/10.1371/journal.pone.0232878
Please Sign in (or Register) to view further.